Suggestions on Picking a Donor
Originally posted March 25, 2025
I know picking a donor can be a very hard thing. It’s a big decision that will both effect whether you have a baby and then the remainder of your and your child’s (and hopefully grandchildren and great grandchildren’s) lives forever. And even more so that other major decisions, it is one where the amount of information you know for sure is much less than you would like.
Nonetheless, I do think that there are better and worse ways to at approach the decision. And most recipients (along with their doctors and partners and friends) are not very smart about this because they fixate on very remote risks and superficial things.
Being smart about a donor means applying the same thought process you would use in a more normal consumer decision, say buying a car. It means asking questions about the likely — such as how good is the cars performance in normal driving, do I generally like the appearance, are previous customers happy? These are much better questions than how much would a lightning strike hurt the car or does the car come with pinstripes or do I approve of the politics of the manufacturer’s CEO. My sense is that most recipients focus more on the second type of questions that the first though.
Things to Focus On: Feasibility and Heritability
Recipients and their future children would be better off if they focused much more on two questions 1) can this donor get me pregnant and 2) what HERITABLE traits does this donor possess?
For the first question (can this donor get me pregnant) I would recommend that recipients prioritize proximity and prior success. You are more likely to wind up with a baby if you have a donor who you can get sperm from relatively easily, and who has fathered another child in the recent past. Sometimes recipients say things like “location doesn’t matter we are willing to drive up to 9 hours” presumably because they think they will only need to do so once. Unfortunately this is not realistic, as generally it will take at least a few tries (and likely many) to succeed, and the right time will often come at unexpected times. Male fertility is not well understood so the only way to know that a donor is fertile is if he has succeeded in say the past 3 years. So you are best off with someone who is close by, who seems committed and unlikely to flake, and who has biological children.
If there is just one donor that passes question one, I would stop there and try with him. Don’t waste time holding out for another donor, don’t let the perfect be the enemy of the good. But if you have multiple options that fit the bill than try to think about what traits the donor has, how heritable they are, and how advantageous (or disadvantageous) they could be for your child. By this I am not referring to unlikely genetic diseases (more on that below in the overrated concerns section) but everyday traits; your child’s life will certainly be effected by their height or whether they are a moron; the odds of both of which will be greatly effected by your choice of biological father.
In thinking about this, the concept of heritability is key. Assuming that you are not planning on doing any coparenting, what the donor is providing is simply his genetic information. These genes will be important (or not) to the extent that they influence (or don’t) traits in any child. Heritability is commonly expressed as a proportion or percentage ranging from 0 to 1 (or 0% to 100%). A heritability of 0 means that genetics plays no role in the variation of a trait, while a heritability of 1 (or 100%) indicates that all variation in a trait is due to genetic differences.
Several methods are used to estimate heritability, including twin studies, family studies, and genome-wide association studies (GWAS). Twin studies are one of the most traditional methods for measuring heritability. These studies compare the similarity of traits between identical twins, and fraternal twins. If a trait is more similar in identical twins than in fraternal twins, it suggests a stronger genetic component. Family studies extend beyond twins and examine the resemblance of traits among relatives of varying genetic relatedness, such as siblings, parents, and children. And genome studies use big data techniques to look at large groups of people with known genetics.
Below is a table with some estimates about how heritable different characteristics are, along with my personal view of how important they are likely to be in a person’s life. My recommendation would be to focus on the top part of the table. In particular intelligence is both highly heritable and important to your child’s life prospects (though maybe less so in a future of very wise AIs). There are more heritable traits (such as height and myopia), but unless your child is likely to be in the NBA or you have a religious objection to vision correction, these traits are likely to be less important. There are traits that are very important, such as attractiveness or length of life, whose heritability is likely so low that they can be mostly ignored.
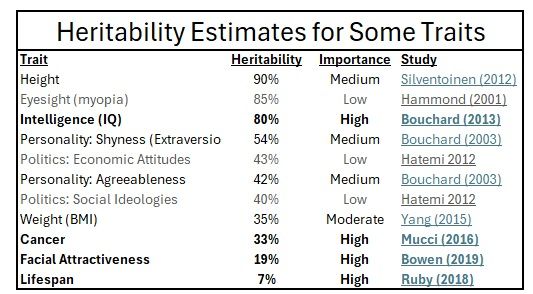
There are many characteristics that are very heritable but few of them are that important. There are many characteristics that are very advantageous to have. But only a few are both. Health might be the most important thing, but the broadest measure, lifespan, appears to be very little influenced by genetics (7% heritability). Attractiveness and cancer, both of which I deem important, are also barely heritable. Conversely, most of the very heritable things like height, eyesight (easily correctable with lenses/Lasik) and eye color have a fairly small effect on most people’s lives. Personality traits are somewhat ambiguous both in desirability (how much better is it to be extraverted then introverted) and heritability (40%-50%). But general intelligence is clearly both helpful in modern society and strongly influenced by genetics.
Things to Focus Less On: Scare Stories, Remote Risks, and Things That Aren’t Heritable
Above I have talked about things that I think recipients should focus more on. But to focus more on one criteria necessarily means focusing less on another one. If proximity is the most important thing, than it follows that a donor who is much closer should be preferred over a much more distant donor with another thing going for him. All recipients want the perfect donor who checks all their boxes. But that may well not exist in the real world. In particular, the following categories are things that I think most people overfocus on, often dramatically so..
Appearance – Humans are very visual and, to state the obvious, physical attractiveness is very attractive to us. Everyone wants to have the cutest child. While the benefits of being very good looking may be temporary and somewhat overrated, obviously it is an advantage we all want for out children. So it is natural that a donor’s looks are usually the most important?/main?/only? thing recipients consider.
But I think this gets overdone. As described above, attractiveness is not that heritable. Having a handsome father probably increases the odds of a good-looking son, but not by much. It is probably at least as important to teach the kid how to stay in shape and otherwise maximize their looks. Mixed kids might be somewhat more attractive on average, but there is a lot of variance here, and of course other considerations.
One of biology’s little tricks is that you (and your partner if applicable) is going to think your baby is the most exquisite and cutest thing ever, even if no one else really does. How many times have we all seen Instagram posts from a mother with an um irregular looking kid with her bragging about how gorgeous the poor little guy is. So don’t worry so much what they look like are going to look like at six months. You can’t really predict that very well regardless of who the donor is, you probably won’t know the difference, and whatever it is (more or less attractive) very well might not last.
STD Worries – This is going to be controversial and easy to misconstrue. Of course all donors should give their recipients clean and relatively recent (say no more than six month old) STD tests. If they are a regular donor they should already have this, and if new they should be willing to test (possibly at the recipients expense). Personally, I test roughly quarterly, have never had an STD and practice safe sex in my fairly sedate private life. Having said all that, many recipients think that avoiding STDs is the main thing to focus on. This causes them to go with frightfully expensive but otherwise inferior frozen clinic sperm rather than go against their (self-interested) doctor’s bad advice that doing otherwise risks an STD.
Even if a donor contracted an STD since his last test, it would be fairly hard for him to pass it on, particularly with artificial insemination (e.g. no sex) since many STDs are not thought to be transmitted by semen alone. The FDA mandates that clinic donors test for HIV, Hepatitis B & C, HTLV, CMV, Syphilis, Chlamydia and Gonorrhea. Even with sex, which involves far more intimate and prolonged personal contact than AI, the per-encounter risk of contracting most STDs is surprisingly low.
For HIV, the risk that a woman contracts HIV from unprotected sex with someone who has HIV is under 1 in 1,000. For Hepatitis B the risk is ridiculously low, with one study estimating it to be less than 1 in 380,000! For Hepatitis C I didn’t find a study but the Mayo Clinic says the risk of heterosexual transmission is “very low — unless you also have human immunodeficiency virus (HIV)”. CMV is not normally considered an STD as it is mostly transmitted from young children via saliva. It is likely only transmissible in sex during an acute infection and accordingly even men who test positive for CMV antibodies (but are likely not still contagious) are allowed to be donors.
For Syphilis, the transmission risk in intercourse is much higher, but this is usually due to contact with a sore, not the semen. HTLV does seem to be spread by semen. But it is a relatively minor disease and has not been studied as extensively. As a retrovirus similar in structure (but not severity) to HIV, maybe the 1 in 1000 risk for HIV is reasonable for it as well. HTLV is also quite rare in the USA. ChatGPT says that 0.1-0.2% of Americans have it, but most don’t even notice.
That leaves Chlamydia and Gonorrhea. Both of these are spread mostly through semen, and so are a legitimate risk in both NI (sex) and AI. Though I emphatically have no experience here, I’m sure they are both unpleasant. But they (along with syphilis) are also easily treatable with a course of antibiotics.
I’m not trying to dismiss the necessity for STD testing. By no means should you use an AIDS patient as your sperm donor! But for the reasons above I do think it is misguided when recipients get very hung up about testing. For instance, sometimes a recipient will say “it has been a month could you get another test” or “can you take a rapid test in front of me” or “how do I know you didn’t fabricate this”. To me, those are semi-red flags, partly because the risk is so low, but mostly because I think they belie a kind of negative mindset, paranoia and lack of trust that could be problematic to both myself and the child IF I succeed in helping her get pregnant.
Number of Donor-Siblings/The Incest Thing – Many recipients make a big deal about this, usually wanting their children to have as few donor-siblings as possible and frowning upon prolific donors. I think this is based on an underlying instinct towards exclusive pair-bonding that is not applicable in the donor context. And frankly I think there is a lot of selfishness to it. The recipient wants to find the best donor, have him help her, and then prevent him from helping other women with the same need in the future. And the whole time she may be complaining about how hard it is to find a donor.
People generally dress up what I think is a baseless “too many siblings” concern by pointing to risk of consanguinity, e.g. unknowing incest. Two donor siblings are going to unknowingly fuck and all then all hell is going to break loose. As I have written about previously, the odds of this happening are so low that it can basically be ignored. The world is simply too big, with too many potential mates, for this to be likely. Not to mention the fact that most donor conceived people know they have donor siblings and often know many details about their donor (especially the non-clinic ones). They will be much more likely to be hit by lightning than to bang a donor sibling.
But say somehow, the consanguinity risk materialized. How big a deal would it be? From the amount of stigma you would think this must be an absolute cataclysm, maybe somewhere between letting an engineered virus escape from a BSL-4 laboratory and crossing-the-streams in Ghostbusters. The reality would actually be pretty tame; if two donor siblings unknowingly produced a love child, that child would have a modestly higher risk of a genetic disorder. But most likely it would be a perfectly normal child. And advances to gene therapy treatments may well provide cures over the next 15+ years as well.
Donor-sibling are genetically half siblings. This is a close genetic relationship. But it is not that close; half-siblings share 1 in 4 of their genes. In comparison, first cousins share 1 in 8. While in current American society it is not acceptable for cousins to date, it once was, and very much still is in parts of the world. The term “kissing cousins” exists for a reason. Today we tend to assume that this type of “incest” will produce genetic monsters with three heads. But that is hardly the case. Paul Samuelson, one of the towering intellects of the last hundred years, was the product of a cousin marriage. Albert Einstein’s second wife, Elsa (nee Einstein) did not have to change her name when they married because she was a second cousin on his father’s side AND a FIRST cousin on his mothers. They did not wind up having any kids, likely because she was 42 when they married, but there is no evidence that Einstein did anything to prevent it (were condoms even legal in 1919 Switzerland?). Charles Darwin produced four healthy (and mostly successful) children with his first cousin Emma Wedgwood.
In many places cousin marriage has been strongly encouraged. In modern Pakistan as many as 60% of marriages involve cousins. When that many marriages involve cousins on one side, it stands to reason that many will involve cousins on both sides. And do you know what the genetic relationship is between first cousins on both sides? You guessed it, it is 1 in 4, or exactly the same as between donor siblings. If anything this understates the level of consanguinity in Pakistan because it is not just the parents that are likely cousins, but the grandparents and great-grandparents as well. Pakistanis suffer a higher rate of genetic problems, but it is by no means pervasive or problematic enough for the cousin marriages to be curtailed even in some diaspora communities. To put some numbers to this, one study found that in Pakistanis (80% of whom had cousin parents), 4.6% tested positive for a genetic condition. This is around twice what you would expect in any population.
Don’t get me wrong, I’m not advocating being a brother-fucker or a kissing cousin. I’m just saying that consanguinity risk is farfetched and inconsequential. It is exactly as big a deal as any recipient (or donor conceived person) chooses to let it be in their lives.
What will really matter to your child is A) WHETHER THEY COME TO EXIST AT ALL and B) what attributes they possess. I wouldn’t recommend letting paranoid delusions about a (non) problem worsen their prospects on either score.
Resemblance to Other Parent – Obviously you and your partner are free to do whatever you want here and there is no wrong choice. If your partner is a red head with dimples and increasing the odds that the child shares those features is important to them (or you are the red head partner and it is important to you) that by all means try to find the donor who fits the bill. Just be careful that you don’t tradeoff too much in terms of the likelihood of finding a donor as well as other heritable traits. Unless you are in a heterosexual couple in need of donor sperm, everyone is going to know that the child is not biologically both of yours. And you will also, dimples or not. Relationships are not normally about shared looks, as any committed adoptive or step-parent can attest. Most adults who raise a baby will instinctually come to love it and quickly look beyond resemblance fairly quickly.
One of my first successes was with an inter-racial (black and white) lesbian couple. I helped the black one, so they have a mixed child. When the white one was looking for a donor, having that donor be black so the children would “look alike” was of paramount importance to them. They should absolutely do whatever they want and I recognize that racial identity is a fraught topic. I hope that they succeed and the two children wind up with a close relationship. That said, by going with a different donor, they ensured that the children would have no biological relationship. They may get children who have a similar hue but are otherwise much more dissimilar than could have been the case. Steve Jobs’ experience is at least interesting. He was adopted as an infant and raised with a sister with whom he shared no genes. According to Walter Isacson’s excellent biography, they were never close and had little contact once he left home. Meanwhile, as an adult, Jobs met his full genetic sister, the author Mona Simpson, for the first time and they quickly became and remained very close.
Rare Genetic Diseases – A lady in a Facebook group once asked me what I would recommend looking for in a donor. I said I’d consider heritable traits. And she responded, “yes of.course I’m going to make sure that they won’t give my kids a disease”. But that is not what I meant at all. We all get much more than the presence or absence of acute disease from our genes. I was talking about the heritable traits described that the child will DEFINITELY possess in some way (though not solely due to their genetics) not the remote possibility that they are will get a genetic malady.
It might be a good idea to get genetic testing done yourself and ask for that from a donor, particularly if you both share a high-risk background. Or if you already know you are a carrier of something relatively common like cystic fibrosis. With my Jewish heritage, I did both 23andme (cheap and easy) and the much more comprehensive Invitae 500+ condition one. But you can probably wait till after you get pregnant to worry about this. After all that is what most conventional couples do. If the donor does not have genetic screening it probably isn’t worth spending a lot of money (or a lot of even more precious time) getting tests since you may not succeed with that particular donor.
Donor’s Interests, Politics or Hobbies – This kind of stuff is unlikely to be heritable. Unless you plan on making the donor a part of your child’s upbringing, these donor attributes will not impact the child’s life. Worrying about this is like letting Elon Musk’s politics influence whether you buy a Tesla. Some people do it, but it is silly and leads to poor choices. If a Tesla is going to be best for your lifestyle than you should buy it even if you dislike Elon’s politics. And if there is another car that is a much better deal, you should buy that one, even if you are a huge fan of the Department of Government Efficiency. Doing anything else is just hurting yourself, and maybe in this case your future child.
This has been a very long post so I doubt anyone will get this far. But if you do I also refer you to the incredibly altruistic donor Drew Sollenberger’s thoughts on what to look for in a donor. I don’t necessarily agree with all of it, but in general it is excellent, particularly in its discussion of not believing donors who boast about their fertility.